
Light induced visual-response: Objective, functional vision testing

Light induced visual-response (LIV)-the use of light to stimulate electrical responses from cells within the eye-has recently emerged as a better way to describe visual electrophysiology testing.
There is an old perception that electrophysiology is mostly used to detect esoteric eye disease and for monitoring subtle changes in rare pathologies in the institutional setting.
In reality, modern LIV tests can help guide clinical decision making in pathologies that we see on a routine basis by using streamlined protocols and platforms which fit into the practice setting.
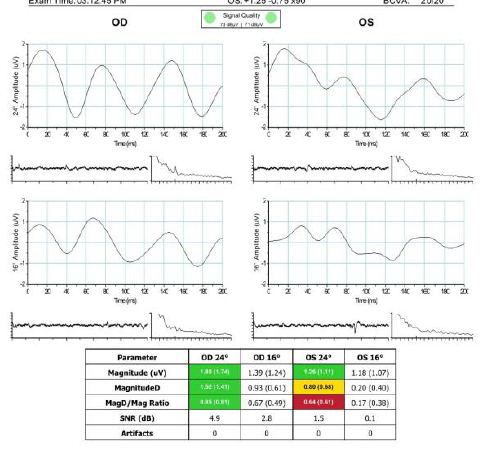
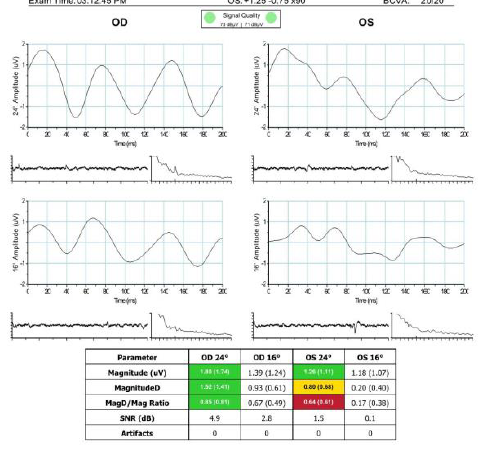
Modern LIV platforms do not require a PhD level of technical understanding. The reports generated by my in-office platform use green-yellow-red color-coding to note healthy, caution, and likelihood of pathology, respectively (Diopsys).
The testing is comfortable for patients, does not require a contact lens, and is more patient-friendly than a visual field.
Additionally, using LIV has not negatively impacted our efficiency. We have a designated technician who performs all necessary testing, including OCT, visual fields, and LIV. At the same time, the platform we use has a template for running the chosen test that integrates with our electronic records systems for generating reports, patient follow up, scheduling future tests, and integration into coding and billing.
Clinical studies have long supported the use of these types of objective, functional tests for common ocular pathologies, and now modern devices make the technology accessible to the practice.
Diabetic Retinopathy
Flicker electroretinography (ERG) is a type of LIV that uses a fast flashing light to stimulate cone cells. Flicker ERG can help stage patients with diabetic retinopathy (DR),1-5 and with the recent availability of anti-VEGF therapy for treatment of DR, it adds additional clinical relevance.6
Treatment of DR in the absence of diabetic macular edema (DME) is discretionary; serial LIV testing to objectively monitor the function of the retina may indicate decline before progression is evident on other imaging (including OCT and angiography).
Certain clinical features, such as cotton wool spots, exudate, dot and blot hemorrhages, microaneurysms, and early IRMA, indicate a risk for DR progression. Closely monitoring patients with these signs using flicker ERG is beneficial for deciding when to start intravitreous anti-VEGF injections. Over time, flicker ERG output helps time the treatment intervals and may suggest a possibility of stopping therapy once stable disease has been achieved.
Flicker ERG can simplify the approach to patients with DR by stratifying patients with mild, moderate, or severe nonproliferative DR, and thereby use this objective information regarding the function of the retina to determine treatment in the first two categories of patients.
Age-Related Macular Degeneration
Similar to DR, clinical features will indicate a role for performing ERG in patients with age-related macular degeneration (AMD). Performing testing in a patient with stable dry AMD may be excessive.
However, if soft or confluent drusen are present, or if there is an increase of macular thickness on OCT, testing the function of the retina is relevant.
Certain other risk factors (hemorrhage, health of fellow eye) may also suggest a high proclivity for developing neovascularization or conversion from dry to wet AMD. Establishing the baseline function of the retina and following that over time with flicker ERG is thus potentially prognostic and diagnostic, and it also provides an individualized endpoint if any treatment is initiated.
Glaucoma
An important application of LIV is in patients with glaucoma. Glaucoma is an optic neuropathy characterized in its early stages by the death of ganglion cells, and therefore it makes sense to objectively measure function as an index of ganglion cell viability. Pattern ERG is a type of LIV test which uses a pattern stimulus to induce an electrical response from retinal ganglion cells.
While monitoring patients with ocular hypertension or suspect glaucoma, pattern ERG provides the earliest indication that ganglion cell viability is compromised relative to visual field and OCT.6
Pattern ERG can also be additive in diagnosing progression.
For example, in a patient with suspicious discs, moderately elevated pressures to the low or mid 20s, and no visual field changes, serial pattern ERG testing may be useful as a diagnostic tie breaker. Any change from the individual’s initial results may indicate an opportunity to intervene, even before a visual field deficit has can be seen.
Just as important, the pattern ERG signal can improve after treatment. At a biologic level, this is an indication that treatment started when the ganglion cells became unhealthy, but before they died. LIV results can show our patients we are not just preventing further damage, but we intervened early enough to help improve function.
Conclusion
LIV is a proven diagnostic tool that has been around for several decades. Modern devices now provide the technical capacity to offer LIV testing to more patients with no tech-learning curve, and easy clinician interpretation.
Disclosures:
Steven M. Silverstein, MD, is president, Silverstein Eye Centers in Kansas City, MO. He is a speaker for Diopsys.
References:
1. Bresnick GH, Palta M. Temporal aspects of the electroretinogram in diabetic retinopathy. Arch Ophthalmol. 1987;105:660-664.
2. Holopigian K, Greenstein VC, Seiple W, Hood DC, Carr RE. Evidence for photoreceptor changes in patients with diabetic retinopathy. Invest Ophthalmol Vis Sci. 1997;38:2355-65.
3. Kim SH, Lee SH, Bae JY, Cho JH, Kang YS. Electroretinographic evaluation in adult diabetics. Doc Ophthalmol. 1997-1998;94:201-13.
4. Pescosolido N, Barbato A, Stefanucci A, Buomprisco G. Role of Electrophysiology in the Early Diagnosis and Follow-Up of Diabetic Retinopathy. J Diabetes Res. 2015:319692.
5. Tzekov R, Arden GB. The Electroretinogram in Diabetic Retinopathy. Surv Ophthalmol. 1999, 44:53-60.
6. Banitt MR, et al. Progressive loss of retinal ganglion cell function precedes structural loss by several years in glaucoma suspects. Invest Ophthalmol Vis Sci. 2013;54:2346-2352.
Newsletter
Keep your retina practice on the forefront—subscribe for expert analysis and emerging trends in retinal disease management.








 in wAMD, DME, and DR")

