
News|Videos|March 3, 2026
EYLEA 8mg in RVO: QUASAR clinical perspectives video
Advertisement
Episodes in this series

Prof Gale: So, the 64-week data that maybe the headline of it is the improvement in visual acuity. Could you explain to us how you feel that the improvement of visual acuity stacks up for our patients and against other clinical trials?
Prof Chaudhary: Patients certainly achieved non-inferiority in terms of what has traditionally been a gold standard with RVO, which is monthly anti-VEGF treatment with a very robust agent like 2mg. So with 8mg, we were able to achieve non-inferiority and that was met even at Week 64 with 8mg compared to 2mg with 2 to 3 less treatments. And it's also important, Richard, as you know, the 64 weeks, if you think about it in years, it's a year and three months. That's a very short period of time and to see a reduction in 2 to 3 injections over that time, I you know, we can both all translate how that will impact patients in the second, third years and beyond. So, once again, I think we're seeing a very significant reduction early on and I think that's going to have a very important impact for our patients while, and this is critical, achieving optimal vision and visual outcomes for our patients.
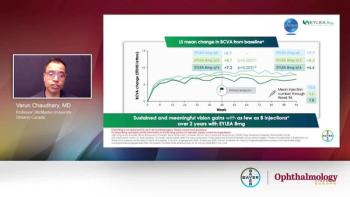
Prof Gale: Yeah, so those those gains that we saw at the primary endpoint at Week 36 was about 17 to 18 ETDRS letters, they were maintained out. So you know, if we think about that, that’s about a 3 to 4 letter line on a traditional chart isn’t it? And that's a really quite a significant improvement in in vision for individuals. But I guess it's not just about vision. We need to have a sense check on that and ensure that the the biomarkers the retinal biomarkers, particularly central retinal thickness, is correspondingly improving at the same time. Would you like to describe how how that looked in relation to the visual acuity?
Prof Chaudhary: I certainly was very impressed with the with the CRT findings with aflibercept 8mg and the concern, two key concerns for me is ‘a’ is we want to see a rapid reduction in CRT, and then we want to see a sustained level throughout the study. And at least for me, Richard, I think the study accomplished that very well. There was some minor fluctuations in fluid, I think the maximal fluctuation was 30μm, so it that's relatively small over a study that’s 64 weeks, and this fluctuation got better with time. I am, you know, very confident in terms of disease control we see in terms of CRT change and and reduction in CRT and again, this was achieved with fewer treatments. So, I I certainly was impressed by it Richard. Your your thoughts in terms of the anatomy and the anatomic outcomes.
Prof Gale: Yeah, so I think there's there's a couple of interesting points here. I think the speed of resolution. So as you mentioned, this is a really high anti-VEGF state disease and perhaps this is a really good opportunity for a medicine to test its mettle against that high VEGF state. And we see those rapid reductions and you know I think there's about a 350μm or so reduction even out at Week 64, and that’s a really substantial reduction within the central retina retinal thickness and that was controlled all the way through. As you say, there was a a minor fluctuation, I think it was about 25μm, and that was in one particular group. And that group was the 8mg group that was treated with three initial monthly doses and then was extended to 8 weeks there afterwards. And we saw about 25μm increase but I think that's probably not clinically significant. And I think, you know, in our real-world practice, we would pick up any minor fluctuations that we would see, as well. So I just wanted to touch on a really important aspect you mentioned which was the reduction in the burden. And you know, the number of treatments which were within, seen and observed in the trial out at Week 64. So there were about 11.2 mean injections given in the 2mg group but in the 8mg group, certainly 8q8/3 group, there was 8.5 8.5. What does it what does that mean to you? Perhaps, what does that mean to our patients, about, you know, a 2 or 3 numerically reduction in intravitreal injections over that time period?
Prof Chaudhary: I I think, Richard, you, I and I'm sure all clinicians can relate to telling a patient that we are going to skip an injection or even to extend an interval. The smile on the face the the the the the smiles on the family member's face, this is, you know, it's it's it’s highly, stressful time for patient to go through treatment and also difficult for family members to bring them to clinic visits. So I think it's extremely important to be able to reduce the treatment but I think not at the expense of losing vision or poor control. And I think that's the key here. You know, the DRM criteria that were used in in the in the study allowed us to achieve that goal of reducing treatments while achieving optimal outcomes. And I at least find the DRM criteria very easy to replicate. That's always been a challenge in taking these explanatory Phase III trials and bringing them to our practice and reproducing the results. So I wanted to ask you, Richard, what are your thoughts in terms of do you think, you know, do you are you hopefully going to achieve the QUASAR results in your practice, both from a personalised treatment perspective and also from a subgroup perspective, because we know there's the the BRVO mild BRVO cases but then there's the highly ischaemic CRVO cases. So are you hopeful you're going to be able to reproduce the results from QUASAR?
Prof Gale: Yeah, I hope so. I mean, it's always quite difficult to produce those ideal clinical situations of, you know, the clinical efficacy we see in clinical trial and turn that into effectiveness in our clinical practice. And most real world doesn't quite get there, but it goes it gets close to it. So I'd hope we would get close to it. I mean you make a really good point here about perhaps how those different subgroups of retinal vein occlusion can behave. You know a branch retinal vein occlusion that's relatively non-ischaemic may behave quite differently, may be extended quite quickly with good visual acuity outcomes compared to that very ischaemic central retinal vein occlusion which is very thirsty, very hungry for anti-VEGF as well. So yes, I hope we would but I wouldn’t be surprised if we don't quite get there for the reasons I explained. Now, one of the things that I would hope we’d be able to do is to have less 4-weekly injections and the clinical trial suggested that those 8mg groups only had a very small proportion on 4 weeks. I think it's about 4 to 5%. You know, that's a very low amount compared what we see perhaps with other medications. And indeed that's, you know, about twice or 2 or 3 times less of a figure than we see with it with 2mg. So with the study, it was about 13% that remained on the 4 weeks and I think that speaks to that, you know, four times higher molar dose and perhaps, you know, the reduced ocular clearance that we've we've seen modelled elsewhere as well.
Prof Chaudhary: And I would add to that, I think in at least my clinical practice, I probably have more patients requiring monthly, and because monthly is quite never monthly, monthly is 4, 5, 6 weeks. And again, that is a component of undertreatment because the treatment burden is so high, you don't get a disease under control and then these patients keep coming back because you never achieve good disease control early. So I'm actually quite excited about that patient group as well which is is high treatment need patients because I think being able to extend them quickly will allow us to optimise outcome for this patient. And these are the patients I think, you know, we we get tired, patients get tired and we just extend them because they're just tired of coming in frequently and I think if we can give them fewer treatments but optimise the outcomes, I think that'll be a certainly a a a paradigm shift for how these that subgroup of patients does in our practice.
Prof Gale: Yes, I agree with you. And it's not I mean, as we mentioned before, it's not just those and relieving the burden on those 4-weeklies, it's about how far we can get individuals out. And this you know, this trial enabled individuals to get out to 16 weeks and even potentially be assigned 20 weeks. Around over 50%, in fact, in in some of the 8mg groups who were being assigned or even achieving those longer intervals as well. And again, that's really meaningful for I think, for patients in in planning their lives and and for ourselves planning our clinics, which are often strained and burdened as well. So, look, Varun I'm really interested in visual acuity, I'm really interested in central retinal thickness and relieving burden, but I'm equally interested in the safety of all of the medicines that we use. In fact, one of the first things I look at when I'm reading a fresh paper or looking at looking at results. Would you like to perhaps comment on the the safety the ocular safety that was reported at the 64-week results.
Prof Chaudhary: You know, it was great Richard, to to look at the ocular safety and and really see what we've seen with 8mg in other indications and and in our clinical practice. There's absolutely no new signals, 8mg’s safety profile in terms of an ocular perspective was comparable to 2mg, which has really been become the gold standard when we look at safety. If you had over a decade of experience with 2mg and there were absolutely no new safety signals, and very importantly, there were no new or no single, not even single case of occlusive retinal vasculitis, which is, of course, one of the key complications that we pay attention to when we look at new treatments coming to the market.
Prof Gale: Yeah, that's really reassuring isn’t it. And I guess it's not just the ocular safety, it's also the systemic safety as well. So retinal vein occlusion we know through epidemiological studies is associated with cardiovascular risk factors and and that's potentially associated with, you know, stroke, heart attacks, these APTC events as well, and I was really pleased to see the the that was recorded, there's a lot of attention paid to that. And there was no differences in balance between the 2mg, the established 2mg and the 8mg group as well. So I think that's really quite reassuring as well. Would you would you agree or do you think, you know, ultimately, do we need to collect more data to reassure us?
Prof Chaudhary: I mean, certainly I think, you know, with any new treatments we will need to monitor this and I'm sure, the companies themselves and and us as individual societies will be looking and and carefully monitoring for complication like we do with any new treatment that comes to market. But certainly very reassuring that there has been no signals and I think our experience builds on what we've already been seeing with aflibercept 8mg. We've already had a very good go with the agent in practice in patients who have bad diabetes or elderly patient with macular degeneration, and there's really been no concern. I mean, I've had absolutely zero concern about the safety profile and similar to, I think, many of my colleagues. So, yes, we need to pay attention, you need to be on the lookout for any concerns but certainly right now, it seems like things are going very well.
Advertisement
Related Content


Latest CME
















Advertisement
Advertisement
Trending on Modern Retina
1
Retina World Congress 2026: Dry AMD — Geographic atrophy, photobiomodulation, and the road ahead
2
Phase 3 data support OTX-TKI's durability in wet AMD: 1 injection, 1 year
3
Retina World Congress 2026: The dopamine-AMD connection
4
Retina World Congress 2026: Port Delivery System shows durable outcomes at 7 years in neovascular AMD
5