Now Playing
QUASAR is the first Phase III, randomised controlled trial looking at the efficacy and safety of aflibercept 8mg in management of patients with macular oedema from retinal vein occlusion. In QUASAR, patients were randomised 1:1:1. The control arm was aflibercept 2mg given every month, and the 8mg, we were looking for rapid extension, so one arm received three monthly loading doses and then extended out to 8 weeks right away. And the second arm received five monthly loading doses and then extended out to 8 weeks. The primary endpoint in QUASAR was Week 36, and this was a non-inferiority visual acuity endpoint, and the study went out to Week 64. Important to remember that QUASAR had simple, easy to replicate DRM criteria that were used to personalise treatment, so patients who needed more treatment were allowed to get more treatment, and patients who were stable and doing well could be extended appropriately. Patient groups were well balanced at baseline across all three treatment arms.
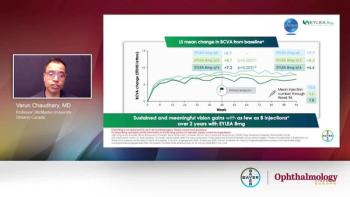
QUASAR met its primary endpoint in that it showed non-inferiority for visual outcomes for both 8mg aflibercept arms, compared to aflibercept 2mg at Week 36. There were rapid and sustained vision gains noted in all three arms, and these were maintained all the way to study end at Week 64, despite needing fewer treatments with aflibercept 8mg. We also assessed CRT and anatomic outcomes. Once again, we saw rapid improvement in CRT and this was maintained in all three arms, including 8mg all the way to study end at Week 64 despite fewer treatments. Secondary outcomes also included number of treatments, and 8mg achieved non-inferior visual acuity outcomes and sustained improvement in anatomy despite fewer treatments. On average, 2 to 3 fewer treatments were required with 8mg compared to 2mg. And I think this is especially important if you think of the duration of the study, which is only a year and three months. So we're seeing a significant reduction in number of treatments over a relatively short period of time and we can extrapolate what this might mean for our patients and their journey in our clinics.
Durability was assessed in a number of ways in the QUASAR study. One aspect of durability was the number of treatments required. The 8mg arm achieved non-inferior visual acuity outcomes with fewer treatments. On average, 2 to 3 fewer treatments were required in the 8mg arms compared to the 2mg arm. I believe this is very impactful because the study was a relatively short study. It was about a year in three months, so even during that short period of time, even with the loading dose, we were seeing a significant reduction in number of treatments and we can appreciate what this might mean for patients in our clinic who come back for many years for treatment. The second aspect of durability was the last treatment interval and, in QUASAR, the 8mg arm, over 78% of patients were at q12 weeks or longer, in terms of the last treatment interval. Lastly, we also wanted to look at durability at the other extreme, which is the treatment-intensive patient group. These are the patients who are needing very frequent treatment. In 2mg aflibercept arm, that was about 13% of patients in the trial. With 8mg, we were able to reduce that to around 4 to 5% to reduce that number of patients by over two thirds with using aflibercept 8mg, in terms of treatment-intense patients. So what we're seeing is a durability signal, not just in those patients who are stable and we can extend longer but in addition to patients who need frequent treatment, we're shifting the curve for those patients as well. So ultimately, I think QUASAR had demonstrated a very strong signal in terms of durability, and this was applicable to all patient groups, as well as the subgroups we looked at, which was the BRVO subgroup as well as the CRVO and HRVO subgroup.
The data from QUASAR is very consistent with what we've seen with 8mg in other indications. There's been absolutely no indication of any new safety signals and the safety profile is very much consistent with what we’re used to, now with over a decade of experience with aflibercept 2mg. And very importantly, there were no cases of occlusive vasculitis in any of the patients.
QUASAR is certainly a paradigm shift in management of patients with macular oedema from retinal vein occlusion for a few reasons. Up until now, all other approved anti-VEGF agents have used monthly dosing to achieve strong visual and anatomic outcomes. With QUASAR, we are seeing for the very first time that we can achieve optimal vision outcomes and sustained vision outcomes and optimal reduction in CRT with three loading doses and early extensions. I think RVO is an ideal condition for early extension because we truly want to personalise treatment in retinal vein occlusion. In RVO, we see VEGF levels are very high, but there's a lot of variability amongst patients. Some patients have a small macular branch retinal vein occlusion, other patients have an ischemic CRVO. So we truly want to be able to personalise treatment as soon as possible so we give the right amount of treatment to the right patient at the right time. And the QUASAR study protocol allowed us to do that in a very efficient way that reduced the number of treatments in a significant manner compared to our standard treatments with 2mg.