
























Studies highlight the need for specialists and training programs focusing on the disease.
Studies highlight the need for specialists and training programs focusing on the disease.

Bradley Smith, MD, presents at AAO 2020 on how fingolimod 0.5 mg, a first-line treatment for multiple sclerosis, may reduce both the number of relapses and disease progression in patients with relapsing-remitting MS as well as the incidence of uveitis.

Glenn J. Jaffe, MD, presents a summary of the results of a confirmatory study on a previous Phase III trial that examined sustained drug delivery for the treatment of uveitis, as well as data on the 36-month results in the second, confirmatory phase 3 study of YUTIQ.

Chronic cases can be difficult for retina specialists; treatment is satisfying.


Inhibition plays role in autoimmune-based inflammation; has unique mechanism of action

One biologic response modifier has indication for uveitis; several in development to gain FDA approval
Quiescence, steroid-free quiescence achieved in VISUAL III trial
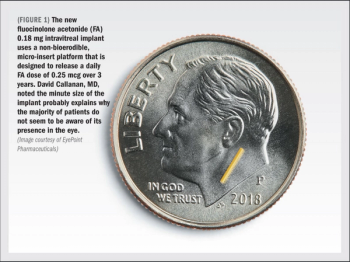
FA implant effective in lowering recurrence rates through available 6, 12 months of follow-up

Improvement in visual acuity, central retinal thickness, vitreous haze reported at 6 months
Intravitreal triamcinolone acetonide, dexamethasone implant superior for regional treatment of disorder



Novel local corticosteroid therapy shows positive efficacy signals, favorable safety profile says Rahul Khurana, MD.


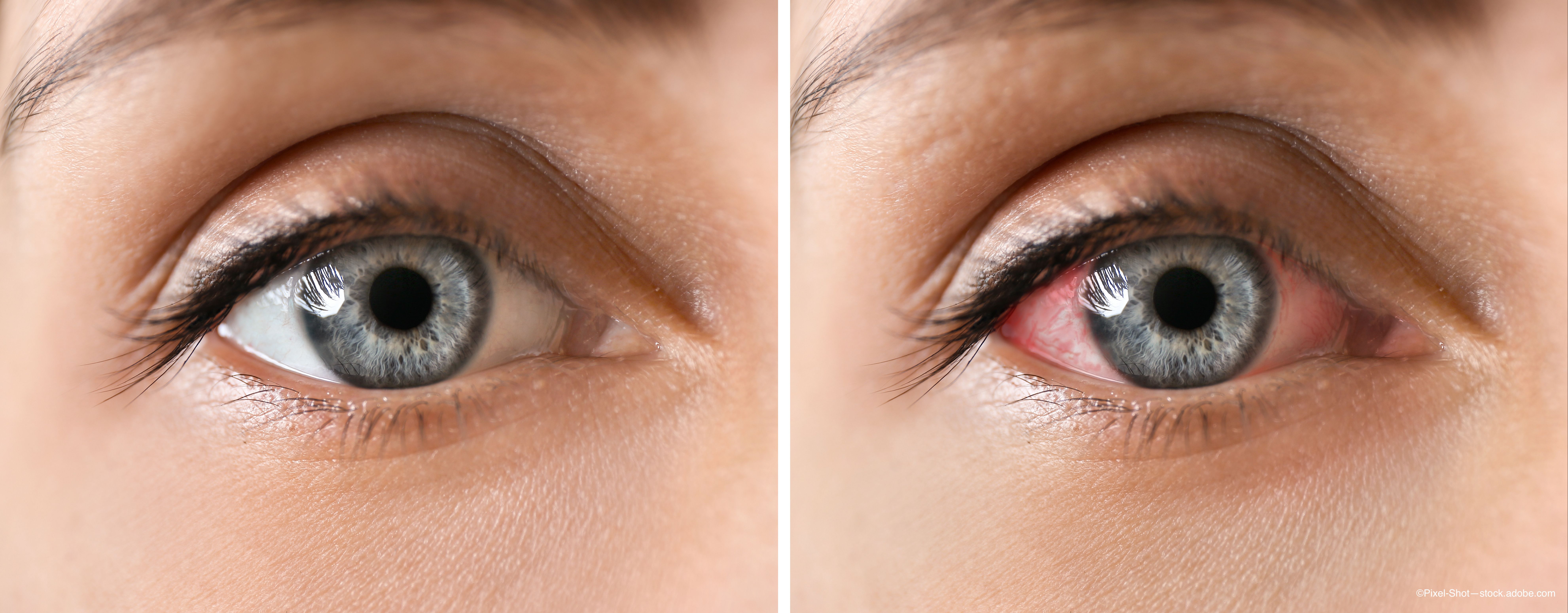
Uveitis does not have to be vexing. Here are some basic principles to make it easier for ophthalmologists to identify the disorder, says James Philip Dunn Jr., MD
Intravitreal sirolimus 400 mcg (Ospiria, Santen) demonstrated positive results in pivotal trials investigating it as a treatment for non-infectious uveitis of the posterior segment. A New Drug Application is under FDA review.
Local therapy plays a significant role in the treatment of uveitis, either as monotherapy or in combination therapy. Alongside a number of pharmacotherapeutic agents, new products and technologies are in development that could expand clinicians’ options and improve outcomes.
Results from the Study Assessing double-masKed Uveitis tREAtrement (SAKURA) program support the efficacy and safety of intravitreal sirolimus 440 mcg (Opsiria, Santen) for treating noninfectious uveitis of the posterior segment, said Pauline T. Merrill, MD.
Results from the Study Assessing double-masKed Uveitis tREAtrement (SAKURA) program support the efficacy and safety of intravitreal sirolimus 440 mcg (Opsiria, Santen) for treating noninfectious uveitis of the posterior segment, said Pauline T. Merrill, MD.
Adalimumab (Humira, AbbVie), an immunosuppressive biologic therapy, improves the symptoms of noninfectious active uveitis, but causes some adverse events and does not cure the disease, researchers say.
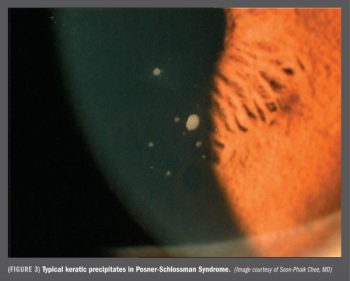
Evidence suggests more ophthalmologists should perform aqueous sampling and viral testing in hypertensive anterior uveitis cases.
Clinicians should recognize the symptoms of West Nile virus, Dengue fever, and Chikungunya that are spread by mosquitos and can have ocular manifestations.
Results of a 6-month phase I/II clinical trial of suprachoroidal injection of triamcinolone for noninfectious uveitis showed the treatment was safe and well tolerated.